
Dermatology Conditions and Treatments
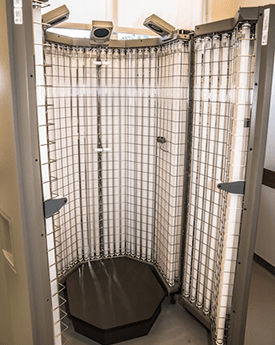
Phototherapy UV patients see noticeable improvement in 1-2 months—twice as fast as biological drugs.
- Evaluation of complex skin diseases
- Immunofluorescence examinations of skin
- Dermatopathology: histopathologic diagnosis of skin biopsies
- Electron microscopy of skin biopsies
- Comprehensive evaluation and management of melanoma
- Comprehensive assessment and treatment of stings and bites
- Mohs micrographic surgical approach to treat large cutaneous malignancies
- Phototherapy and Photochemotherapy
- Patch testing and Photopatch testing
Research Activities
- Mechanisms of cutaneous allergy
- Herpes simplex vaccine
- Jellyfish toxin pathology
- Clinic pharmacology
Special Programs
- Pigmented Lesion Clinic is a multidisciplinary program for diagnosis and treatment of melanoma and following those at high risk for the disease
- Sting and Bite Program uses an integrated approach to identify specimens, examine patients, conduct appropriate immunological tests, treat wounds and identify preventive therapy for patients with stings and bites
Conditions
- Cutaneous manifestations of internal diseases
- Eczema
- Pigmentation disorders
- Psoriasis
- Acne
- Skin cancer and precancerous lesions