
What is Multiple Sclerosis?
Multiple sclerosis is a complex disease of the central nervous system (brain, spinal cord and optic nerves).
It is thought to be an immune-mediated disease, meaning that errors in the function of the immune system cause damage in the central nervous system.
Patients may suffer relapses (neurologic symptoms which appear rapidly but often improve over weeks or months), remissions and often increased disability over time.
MS is currently not a curable disease but effective treatments are available.
The immune system protects the body from various environmental hazards or pathogens, such as viruses, bacteria and fungi. The immune system is very sophisticated and understands the difference between body tissues and outside germs and viruses.
In MS, this is disrupted.
The immune system acts as if the tissue within the central nervous system is a virus or disease, which creates inflammation and damage. Muscles grow weak with no immune system to protect it.
How is multiple sclerosis diagnosed?
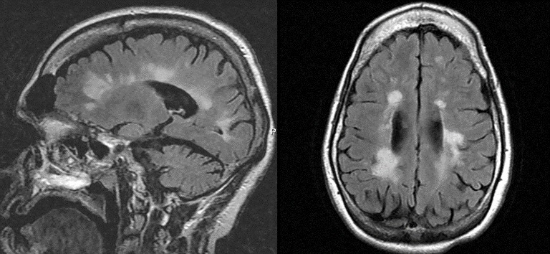
MS is diagnosed based on the patient's history of symptoms over time (if they can be linked to the central nervous system), the neurological examination, and imaging tests such as brain and/or spinal cord MRI. Sometimes other tests are used, such as evoked potentials, optical coherence tomography, and/or a spinal tap.
Blood tests are also used to make sure the symptoms are not caused by something other than MS. As there is no single test for MS, the diagnosis is made by summing together this medical history from the patient.
What are the symptoms of multiple sclerosis?
Symptoms of MS vary among individuals but often include:
- Numbness or tingling in the limbs
- Impaired balance
- Change in vision such as blurred vision in one eye or double vision
- Fatigue
- Change in bowel, bladder and sexual function
- Stiffness or tightness in the muscles
- Weakness
- Trouble walking
How does multiple sclerosis progress over time?
Approximately 85 percent of patients begin the disease with relapsing-remitting MS. These patients experience episodic relapses (sometimes called flares, attacks or exacerbations). They may experience the onset of symptoms over a few days or weeks, with gradual recovery that can be complete or incomplete.
Over time, some patients will experience "progression," less inflammatory changes and more of a slow, progressive worsening of multiple symptoms and disability. This is classified as secondary-progressive MS. Over time there can also be a decrease in brain volume.
Approximately 15 percent of patients never have relapses. Their disease is characterized by an increase of symptoms over time. This stage is known as primary-progressive MS.

